Case Report: 11CA007
Laborer dies when he is crushed by an industrial washing machine
Download a PDF to print this report:
Laborer dies when he is crushed by an industrial washing machine (11CA007, PDF)
Summary
A laborer was crushed by a horizontal drum industrial washing machine while he was reaching into the machine to retrieve clothing. When the machine had first finished its wash cycle, a co-worker aligned the inside door on the horizontal drum of the washing machine with the outside door on the frame. The victim's supervisor opened the drum door, and then the victim began to retrieve laundry by leaning inside the drum. Video shows the supervisor then switched the machine on and the drum suddenly rotated upward, pulling the victim off his feet and pinning his torso between the drum and frame of the washing machine. The supervisor switched off the machine and then attempted to free the victim. Other employees in the shop also came to assist. The door safety interlock was disconnected at the time of the incident. Factors identified in this investigation which may have contributed to the victim's death included the disconnected safety interlock switch and the work practice of one worker reaching into the washer while a second worker was near the washer controls. The CA/FACE investigator determined that, in order to prevent washing machine operators from being pulled into machines, employers should ensure that:
- Comprehensive Injury and Illness Prevention Programs (IIPP) are developed, implemented, and enforced which include worker training in washing machine operations and safety with instructions that are available in the primary language of the user.
- The electrical, mechanical, and safety features of industrial washing machines are maintained or repaired in operating condition, according to manufacturer's specifications. All preventive maintenance should be documented.
Introduction
On Wednesday, July 20, 2011, at approximately 12:30 p.m., a 28-year-old male Hispanic laborer was operating an industrial washing machine when he was crushed by the machine as he leaned into the washing machine drum to retrieve clothing. The CA/FACE investigator received notification of this incident on July 20, 2011, from the Monrovia District Office of the Department of Industrial Relations (Cal/OSHA). On July 27, 2011, the CA/FACE investigator interviewed the employer's safety specialist and two other employee washing machine operators of the company. Pictures were taken of the incident scene and copies of the police, Cal/OSHA, and coroner reports were also obtained. The investigator also viewed employer surveillance videos of the incident.
Employer
The employer of the victim was a clothes processing facility that was involved in various stages of design and production of denim and non-denim apparel through washing, bleaching, dyeing, drying, and processing clothing in bulk. The company had been in business since 2007 and had 40 employees.
Written Safety Programs and Training
The company did not have a written safety program or an IIPP. The company did not have a comprehensive written training program or a visual training aid for the safe operation of the washing machines. The victim was shown how to operate the different washing machines in the facility by a previous supervisor who is no longer employed with the company. All instructions were given verbally to the victim in Spanish on how to operate the washing machines and were not documented.
Worker Information
The victim was a male Hispanic who was born in Mexico and had been in the United States since 2009. He had a fourth grade education and spoke only Spanish. He had worked for the company for three years as a laborer performing various tasks. He had sporadically operated washing machines for the last three years, and he had used the washing machine involved in the incident fewer than six times.
Incident Scene and Machine
The incident occurred in an industrial building that was equipped with 17 large washing machines and 13 drying machines. A low-resolution video surveillance system, installed for security reasons by the employer, monitored various areas within the facility. One camera captured a partially obstructed view of the incident. The machine involved in the incident was a horizontal barrel type industrial washing with a 200-pound capacity (Exhibits 1-4). It was purchased in 2007 when the company changed owners and it did not come with any instructional manuals. The washing machine was manufactured by "Washex Machinery Cooperation" which is no longer in business. There were no markings or identification plates on the machine to determine the machine’s serial number or its age.
The washing machine had two doors to gain access to the horizontal drum. The outside door, which slid upward, was located on the outside frame of the machine. The inside door was located in the center of the drum. It opened upward after it was aligned with the outside door. The process to align both doors required the horizontal barrel to be "jogged" either upward or downward by manipulating the buttons on the control panel. The washing machine also had a safety interlock which was designed to disconnect the electrical power to the motor during wash cycles when the doors were open so that workers could not enter the machine while the machine was running. The safety interlock was inoperable at the time of the incident.
The control panel, mounted just to the left of the machine consisted of an on/off switch and three push buttons (Exhibits 5 & 6). The on/off switch did not de-energize the machine, it simply controlled the wash cycle. The buttons were used to align the inner and outer doors.
According to the victim's supervisor, the washing machine involved in this incident had been out of service for about a six-month period approximately a year prior to the incident. One of the brackets that held the horizontal drum was broken, the drum wasn't aligned properly within the machine structure, and the machine leaked water every time it was used. The employer would only use this machine when the work load demanded it. The supervisor stated that the employer was aware that the safety interlock wasn't working properly.
Investigation
On the day of the incident, the victim was assigned to operate the horizontal drum washing machine and was being monitored by his supervisor. After lunch, the machine finished its wash cycle and a co-worker turned the on/off switch on the control panel to the off position and opened the outside door of the washing machine by sliding it upward, exposing the inner barrel. The co-worker then manipulated the jog buttons on the control panel until the inside door on the barrel was aligned with the outside door opening. The supervisor then came to the machine and the co-worker left to perform other duties. The victim leaned into the washing machine barrel to retrieve the washed clothes. The supervisor then faced the control panel and turned the switch that controlled the wash cycle to the on position. It is not known why the supervisor switched on the machine. The machine suddenly activated and the horizontal barrel rotated upward, picking the victim off his feet and pinning his torso between the barrel and machine frame. The supervisor stated that he heard the victim scream and turned around to see what had happened. He immediately turned the switch off. Other employees came to the machine when they heard the victim scream and attempted a rescue by trying to pry the machine open as well as cutting off the belts that connected the motor to the barrel. Their rescue attempt was unsuccessful. The fire department arrived at the scene and extricated the victim from the machine. He was pronounced dead at the scene. The washing machine was damaged in the rescue operations to the extent that no examination of the machine's function or integrity was subsequently performed.
Contributing Factors
Occupational injuries and fatalities are often the result of one or more contributing factors or key events in a larger sequence of events that ultimately result in an injury or fatality. In this incident, the supervisor switched on the machine and the machine crushed the worker. The CA/FACE investigator identified the following items as possible contributing factors in this incident that ultimately led to the fatality:
- The work practice of one worker reaching into the washer while a second worker was near the washer controls.
- A disconnected safety interlock switch on the washing machine door.
Cause of Death
The cause of death according to the death certificate was traumatic asphyxia and blunt trauma of torso.
Recommendations
In order to prevent washing machine operators from being pulled into machines, employers should ensure that:
Recommendation #1: Comprehensive Injury and Illness Prevention Programs are developed and implemented which include worker training in washing machine operations and safety, with instructions that are available in the primary language of the user.
Discussion: In this case, the victim was given verbal instructions on how to operate the washing machine by a former employee. The victim was not instructed to never use a machine with a faulty interlock and he was not instructed to never reach into the machine if another worker was within an arm’s reach of the controls. In this incident the supervisor manipulated the controls while the victim was reaching into the machine, causing the drum to rotate and the victim to be crushed.
Training in operation and safety of industrial washing machines must be given to all workers, coupled with employer assessments that workers are competent in the recognition of operational and safe work practices. When the victim was hired, he did not receive any type of formal safety training by the employer. The victim was provided verbal instructions on how to operate the machine, but not how to work safely and avoid hazards such as the machine activating when the doors were opened. Training in recognizing and avoiding hazards should be given to all workers, coupled with employer assessments that workers are competent in the recognition of hazards and safe work practices. The training program content and the names and dates of employees completing the training should be documented and retained by the employer. Employers should also ensure that the trainer who provides training is qualified through education and/or experience to conduct the training. To ensure the effectiveness of the safety training, an employer might consider ways to ensure that the worker comprehends the important information (e.g., written testing, verbal questions, or demonstrations). Additionally, employers should provide periodic documented refresher safety training which may be done by conducting on-site toolbox type meetings. If the employer had had a fully implemented IIPP and the worker received training in and assessment of safe work practices, this incident may have been prevented.
Recommendation #2: The electrical, mechanical, and safety features of industrial washing machines are maintained or repaired in operating condition in accordance with manufacturer specifications. All preventive maintenance should be documented.
Discussion: In this incident, the washing machine was poorly maintained and the safety interlock on the washing machine door was disconnected. There was no documentation of a repair request or work completion on the washing machines. Operators would simply tell the mechanic that something was wrong with a machine and wait for him to perform the repair or maintenance. If documentation for the manufacturer's specifications is not available, then any repair or maintenance should be directed by an engineer with knowledge and experience in the operation of that machine. Had the safety interlock on this washing machine been in proper operating condition, the machine would not have started when the supervisor turned the cycle switch, and this incident might have been prevented.
Exhibits

Exhibit 1. The work area where the incident occurred.

Exhibit 2. The industrial washing machine involved in the incident.

Exhibit 3. The industrial washing machine with the sliding door open, exposing the inner rotating barrel.

Exhibit 4. The industrial washing machine opening.
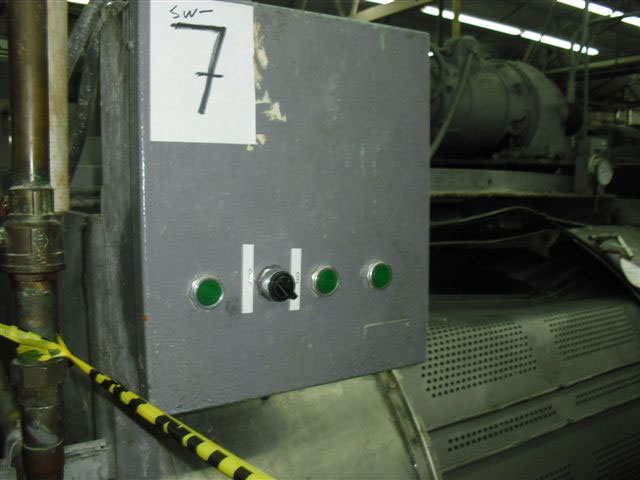
Exhibit 5. The control panel for the industrial washing machine.

Exhibit 6. The buttons on the control panel.
References
Subchapter 7. General Industry Safety Orders
Group 8. Points of Operation and Other Hazardous Parts of Machinery
Article 67. Laundry and Dry Cleaning Equipment -§4481. Washing Machines.
Group 2. Safe Practices and Personal Protection
Article 7. Miscellaneous Safe Practices -§3314. The Control of Hazardous Energy for the Cleaning, Repairing, Servicing, Setting-Up, and Adjusting Operations of Prime Movers, Machinery and Equipment, Including Lockout/Tagout.
Group 1. General Physical Conditions and Structures Orders
Introduction -§3203. Injury and Illness Prevention Program.
Authors
Hank Cierpich, FACE Investigator
Robert Harrison, MD, MPH, FACE Project Officer
Laura Styles, MPH, Research Scientist
June 7, 2013