Case Report: 12CA012
Machine operator in a food processing plant dies when trapped inside a steam pressure cooker
Download a PDF to print this report:
Machine operator in a food processing plant dies when trapped inside a steam pressure cooker (12CA012, PDF)
Summary
A machine operator in a food processing plant died from thermal burns after being trapped inside a large steam pressure cooker. The victim was not visible at his assigned work area so another worker completed his task of moving crates of canned fish into the pressure cooker. The inlet to the pressure cooker was closed, sealed, and then activated by a third worker. When co-workers realized they did not know where the victim was, they began to search for him. After the pressure cooker was turned off and the outlet was opened, the victim was discovered dead inside. The CA/FACE investigator determined that, in order to prevent future incidents, food processing companies should ensure that:
- Periodic safety audits and inspections are conducted and documented to identify all hazardous work areas.
- Employees working in or around confined spaces are properly trained and the training is documented.
Introduction
On Thursday, October 11, 2012, at approximately 5:30 a.m., a 62-year-old Hispanic male machine operator working in a food processing plant died when he was sealed inside a pressure cooker. The CA/FACE investigator received notification of this incident on October 16, 2012, from the Division of Occupational Safety and Health (Cal/OSHA) Bureau of Investigations. On October 22, 2012, the CA/FACE investigator contacted the employer. On November 14, 2012, a joint investigation took place with representatives from CA/FACE, the Los Angeles Department of Coroner, and Cal/OSHA. Pictures of the equipment involved in the incident were taken, and interviews were conducted with employees, supervisors, managers and legal counsel for the company
Employer
The employer of the victim was a food processing facility that processed and packaged canned tuna. The employer had been in business at the facility for 22 years and had 245 employees. There were 120 employees onsite at the time of the incident.
Written Safety Programs and Training
The employer of the victim had a policy and procedure manual which contained the company's written injury and illness prevention program (IIPP), a lockout/tagout procedure, and a confined space entry program that had been in place since 1991 and was recently updated. The steam pressure cooker involved in this incident was not identified as a confined space by the employer. Training for employees working with and operating the steam pressure cookers was mostly informal through on-the-job training (OJT) provided by bilingual senior staff in both English and Spanish. This training did not include recognition of and proper procedures to use in confined spaces.
Worker Information
The victim was a 62-year-old male Hispanic male machine operator who was born in Mexico and had been in the United States for the past 41 years. He had worked at the company for six years and according to fellow employees only spoke Spanish while at work.
Incident Scene
The incident scene was the pressure cooking and sterilization section of a processing plant inside a large warehouse.
Work Process
The machine operator's responsibilities are to load and unload retorts with crates of canned tuna. A retort is a large cylindrical steam pressure cooker used to sterilize and cook tuna in aluminum cans. The cans of uncooked tuna are loosely packed inside perforated carts on wheels.
Both the inlet and outlet doors of the retort are open as the crates are pushed into the cylinder with a pallet jack. After the carts are pushed into the retort, a chain that runs underneath the carts is hooked to the last cart to allow for pulling the load from the outlet side once the cooking process is completed. The inlet and outlet doors are closed and the retort is turned on. When the cooking process is complete, both the inlet and outlet doors are opened and the load pulled out with the chain attached to the pallet jack. The chain is then pulled back through the retort for the next load of carts. According to the employees, the chain would sometimes get snagged or bound within the chain guide and the operator would enter the retort to pull it back through to the inlet end.
Investigation
On the day of the incident, the victim was assigned the task of loading the retort with carts of canned tuna using the pallet jack. When the victim's supervisor went to check on the work progress, he noticed the pallet jack and carts loaded with canned tuna in front of the retort. The inlet door was open and the outlet door was closed. The victim was not visible. The supervisor instructed a co-worker to load the retort while he went to look for the victim. The co-worker loaded the retort with the carts but did not look inside prior to loading. The inlet door to the retort was then closed and sealed by another employee and the steam pressure turned on at 0509 hours. After an extensive search, the supervisor had the retort turned off at 0643 hours and the outlet door was unsealed and opened. The victim was found unresponsive inside the retort by the outlet door and pronounced dead at the scene by responding police and fire personnel.
Cause of Death
The cause of death according to the death certificate was thermal burns.
Recommendations
In order to prevent future incidents, food processing companies should ensure that:
Recommendation #1: Periodic safety audits and inspections are conducted and documented to identify all hazardous work areas.
Discussion: The employer had written procedures for confined spaces and permitrequired confined spaces for other vessels in the plant. However, the retorts were not identified as confined spaces and there were no written policies or procedures for loading the retorts. The company's safety supervisor was responsible for reviewing their safety program annually to ensure its ongoing adequacy, effectiveness and accuracy as well as to identify any opportunities for improvement. This included review of all safety policies, programs, procedures and training records and other available written safety materials. The company safety supervisor never identified the retorts as confined spaces. As a consequence, the employees working with the retorts never received confined space or permit-required confined space training. Had the employer conducted and documented periodic safety audits and inspections that identified all hazardous work areas for employees, the retorts would have been classified as a permit-required confined space. If the retorts had been identified as a permit-required confined space, there would have likely been the proper procedures, controls and training to safely load the pallets.
Recommendation #2: Employees working in or around confined spaces are properly trained and the training documented.
Discussion: Although the employer had trained employees on confined spaces, the retort was never identified as a confined space and the victim had never received specific confined space training on the operation of this particular piece of equipment. In this incident, the victim most likely went inside the retort to retrieve the chain needed for the removal of the carts. The victim did this with the outlet door closed, and did not inform anyone he was going inside the retort. It is not known exactly why the victim went inside the retort with the outlet door closed, but he may have tried to expedite the work process. A co-worker loaded the carts and was not aware the victim was inside with the outlet door closed. Another employee sealed the inlet door and activated the steam but also was not aware that the victim was inside the retort.
The company should identify all workers who are potentially exposed to confined space hazards and provide training to those employees, including engulfment, oxygen deprivation, presence of toxic gases and mechanical and electrical hazards. The company should ensure that the workers understand the nature of confined space hazards and are familiar with standard confined space entry procedures. The training should be provided before an employee is assigned the specific tasks and a refresher training should be provided at least annually or whenever there is a change in assigned duties, in confined space operations or an update in the confined space entry procedures.
Confined space training as well as all other safety training should be documented and kept on file with the employer. All written and oral training should be offered in the appropriate language and literacy level of the employees who are being trained. Supervision through random observation should be conducted to prevent unauthorized entry and ensure that employees follow all written safety procedures and training. Corrective action should be taken whenever an employee is observed performing tasks outside of the company's safety procedures. If the employer had provided confined space training and appropriate controls for the victim and his co-workers, they would likely have followed procedures to prevent the possibility of anyone being trapped inside the retort.
Exhibits

Exhibit 1. The pressure cooking and sterilization section of the processing plant.

Exhibit 2. The large cylindrical steam pressure cooker called a retort.
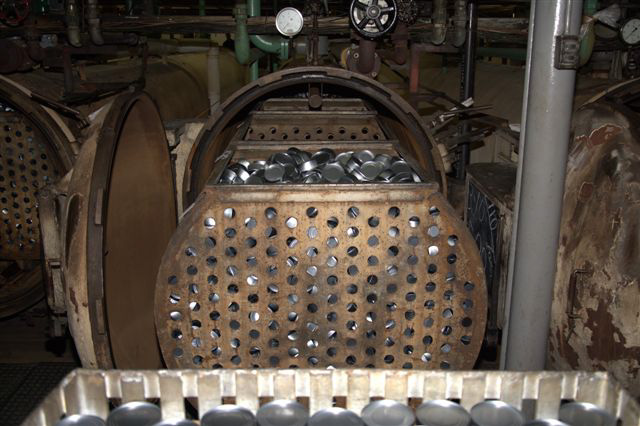
Exhibit 3. Perforated carts filled with canned tuna being pushed into the retort.

Exhibit 4. The chain attached to the last cart.

Exhibit 5. The inside of the retort.
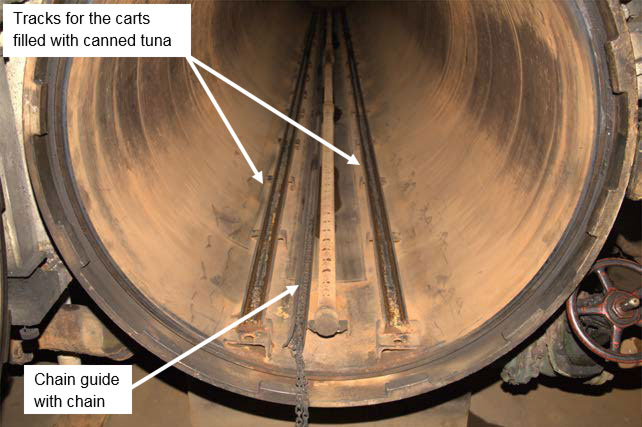
Exhibit 6. The inside of the retort showing the cart tracks and the chain guide.
References
Division of Occupational Safety and Health - Title 8 regulations
Subchapter 7 - General Industry Safety Orders
Group 16. - Control of Hazardous Substances
Article 108. Confined Spaces
§5156. Scope, Application and Definitions.
§5157. Permit-Required Confined Spaces.
§5158. Other Confined Space Operations.
Worker Deaths in Confined Spaces - NIOSH Publication No. 94-103 (January 1994)
A Guide to Safety in Confined Spaces - NIOSH Publication No. 87-113 (July 1987)
Authors
Hank Cierpich, FACE Investigator
Robert Harrison, MD, MPH, FACE Project Officer
Laura Styles, MPH, Research Scientist
April 30, 2014